What if your recurring skin “boils” aren’t actually boils, but a structural systemic failure disguised as a dermatological annoyance? For many patients, the journey toward a diagnosis for Hidradenitis Suppurativa (HS) takes an average of seven years—a period during which the follicular occlusion triad in Hidradenitis Suppurativa operates silently, creating irreversible tunnels beneath the skin. This isn’t a result of poor hygiene or a simple infection; it is a complex pathophysiological cascade that begins long before the first painful bump appears. Understanding this triad isn’t just academic; it is the only way to halt progression and avoid the life-altering scarring associated with Hurley Stage III.
In this clinical deep dive, we move beyond the surface-level descriptions of “clogged pores.” We will explore the three-stage mechanism—hyperkeratosis, follicular rupture, and chronic inflammation—that defines the follicular occlusion triad in Hidradenitis Suppurativa. By the end of this guide, you will understand exactly how these microscopic events lead to macroscopic damage and what precise steps you must take to intervene before the pathology becomes refractory to treatment. This perspective, grounded in dermatopathology, offers insights rarely found in standard patient brochures.
Phase One: Infundibular Hyperkeratosis – The Biological Ticking Time Bomb
The genesis of HS does not occur in the apocrine glands, contrary to historical medical beliefs. Instead, the pathology initiates at the terminal hair follicle’s infundibulum. This first step of the follicular occlusion triad in Hidradenitis Suppurativa is known as infundibular hyperkeratosis. Essentially, the lining of the hair follicle begins to overproduce keratinocytes—the cells that make up the skin’s outer layer. These cells fail to shed correctly, leading to a dense keratin plug that seals the follicle shut. This process is not a passive blockage; it is a structural remodeling of the follicle itself.
Notably, this hyperkeratosis creates a high-pressure environment within the hair canal. While common acne also involves follicle clogging, the HS mechanism differs because it occurs in friction-prone, intertriginous areas like the armpits and groin. Furthermore, the genetic predisposition in HS patients makes their follicular walls inherently more fragile. Consequently, while a normal pore might eventually expel a plug, the HS follicle becomes a pressure cooker, preparing for the second, more destructive phase of the triad. The “scarcity” of this knowledge lies in the fact that most treatments target bacteria, yet the primary issue is this structural keratin dysfunction.
Phase Two: Follicular Rupture – The Immunological Explosion
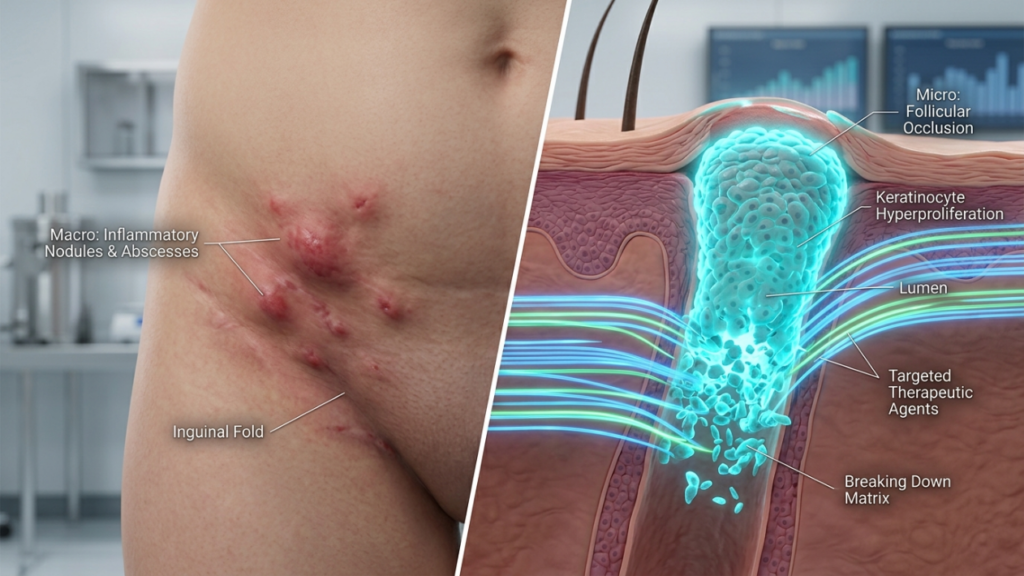
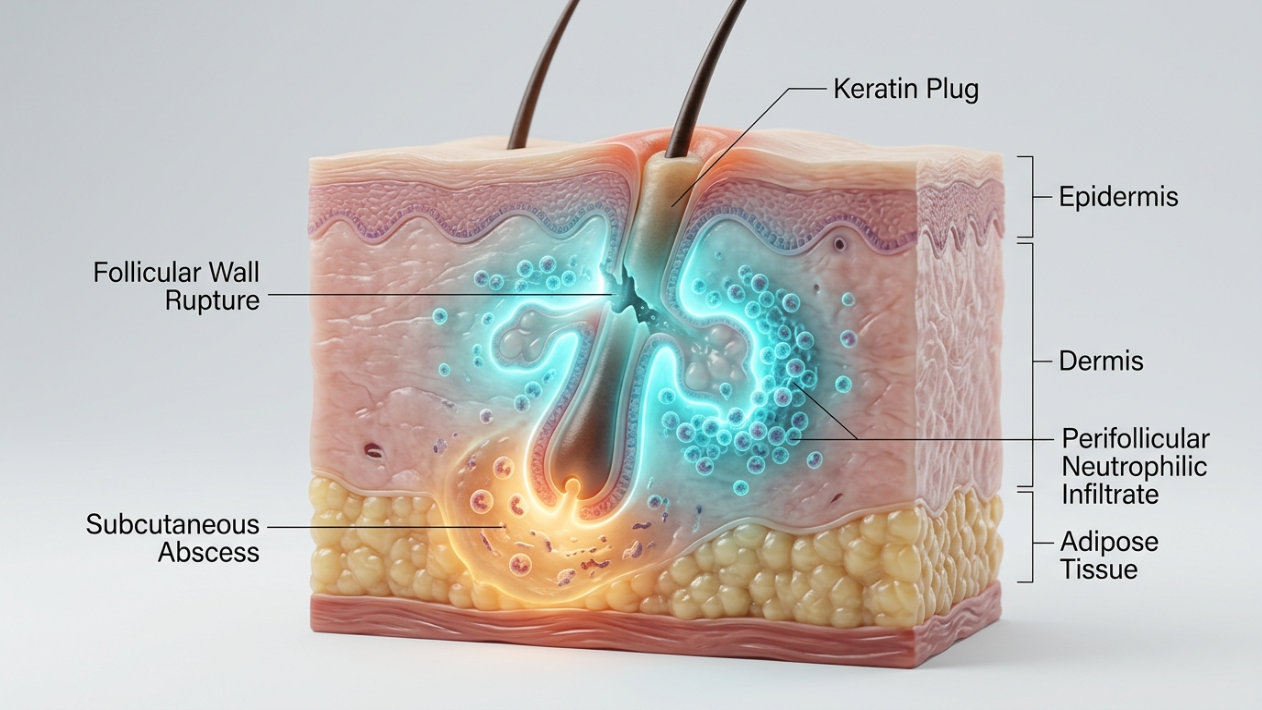
Once the pressure from the keratin plug becomes unsustainable, the follicular wall inevitably breaches. This rupture is the most critical turning point in the follicular occlusion triad in Hidradenitis Suppurativa. When the wall disintegrates, the contents of the follicle—including keratin, sebum, and commensal bacteria—are suddenly ejected into the surrounding dermis. To the immune system, these substances are foreign invaders. This trigger initiates an “immunological explosion,” where the body launches a massive, misdirected inflammatory response.
Specifically, the body recruits neutrophils and macrophages to the site, leading to the formation of an abscess. Unlike a standard pimple that ruptures outward, the HS follicle often ruptures inward or sideways. This internal spill is why HS lesions are so much more painful and deeper than regular acne. Therefore, the goal of early intervention must be to stabilize the follicular wall before this rupture occurs. Once the follicle breaks, the “genie is out of the bottle,” and the disease shifts from a localized blockage to a systemic inflammatory event. This distinction is why topical antibiotics alone often fail; they cannot repair a ruptured structural wall.
The Comparative Reality: HS vs. Furunculosis
Understanding the difference between a simple boil (furunculosis) and the follicular occlusion seen in HS is vital for accurate diagnosis. The following table highlights why HS requires a different clinical approach.
| Feature | Common Boil (Furunculosis) | HS (Follicular Occlusion Triad) |
|---|---|---|
| Primary Cause | Staph Infection | Follicular Hyperkeratosis |
| Recurrence | Random/Sporadic | Chronic & Location-Specific |
| Internal Rupture | Rare (Usually heads outward) | Frequent (Triggers deep inflammation) |
| Long-term Effect | Fades with minor scar | Leads to fistulization/tunnels |
| Response to Antibiotics | Rapid resolution | Partial/Temporary relief |
Phase Three: Chronic Inflammation and Fistulization – The Tunnels of Despair
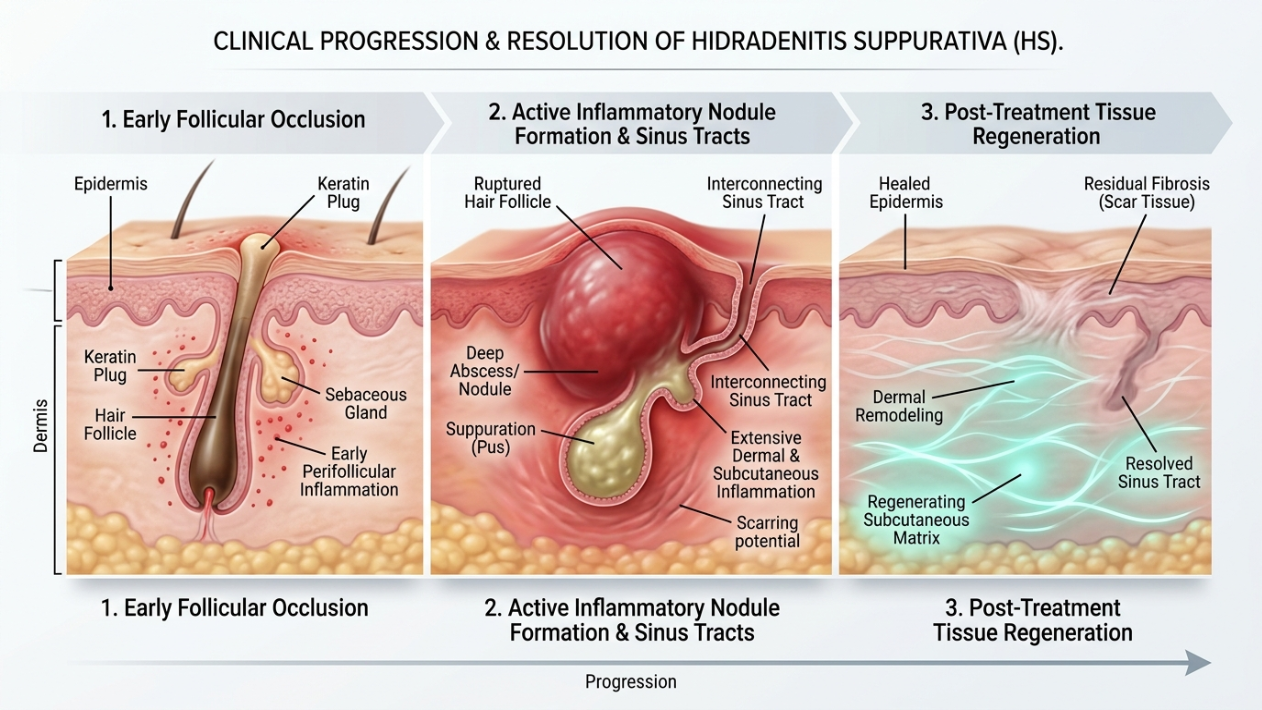
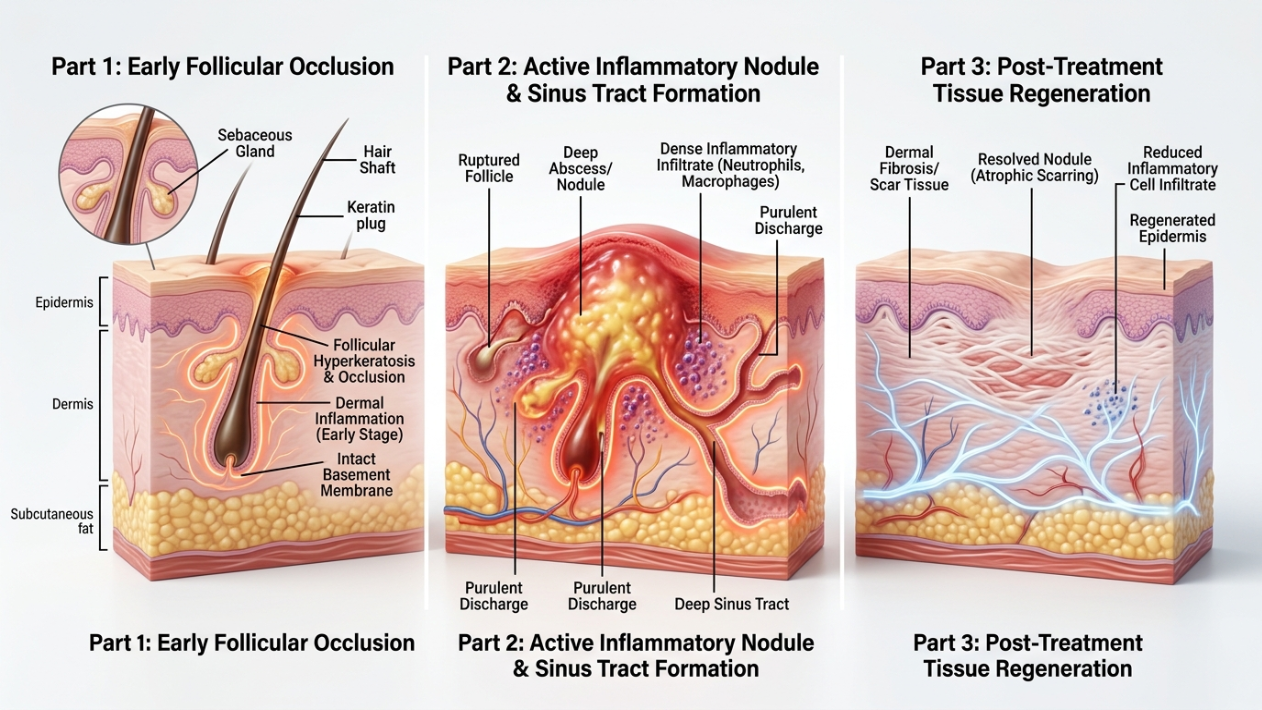
The final element of the follicular occlusion triad in Hidradenitis Suppurativa is the shift into chronic inflammation and the development of epithelialized tunnels, known as sinus tracts. After the follicle ruptures and the body fails to “clean up” the debris, the inflammation becomes self-perpetuating. The body, in a desperate attempt to contain the damage, begins to grow skin-like linings (epithelium) around these inflamed areas. This results in the formation of tunnels (fistulization) that connect different abscesses under the skin.
Crucially, these tunnels are not just passive pipes; they are biologically active and constantly leak inflammatory fluid. This stage signifies the transition to Hurley Stage II or III. At this point, the disease is no longer about individual follicles but about a subcutaneous network of destruction. Consequently, medical therapy becomes significantly harder because the “tunnels of despair” provide a permanent home for inflammation. This is why our dermatology blog emphasizes early detection; we want to catch the triad at phase one or two, where medical management can still prevent the permanent structural changes of phase three.
Hurley Staging Correlation: Mapping the Triad to Progression
The clinical severity of HS is measured by the Hurley Staging system, which correlates directly with how far the follicular occlusion triad in Hidradenitis Suppurativa has progressed. By identifying where you sit on this scale, we can tailor a methodical treatment plan.
- Hurley Stage I: Localized abscess formation without sinus tracts or scarring. This corresponds to the early hyperkeratosis and initial rupture phases.
- Hurley Stage II: Recurrent abscesses with sinus tracts and scarring. These tracts may be single or multiple but are widely separated. This indicates the beginning of the fistulization phase.
- Hurley Stage III: Diffuse or near-diffuse involvement across an entire area (e.g., the whole axilla) with interconnected tunnels and continuous abscesses. This is the culmination of the chronic inflammation phase.
Notably, the speed at which a patient moves from Stage I to Stage III varies based on genetics, smoking status, and hormonal factors. However, the underlying driver remains the same: the unchecked progression of the follicular triad. Every month spent in an untreated Stage I state increases the statistical likelihood of entering the irreversible Stage III phase.
Why Early Diagnosis is Often Missed: The Hidden Pathophysiological Clues
Early diagnosis of HS is frequently missed because the first signs of the follicular occlusion triad in Hidradenitis Suppurativa are subtle. Many patients are told they have “ingrown hairs” or “friction rashes.” However, a trained dermatologist looks for specific clues that point toward the triad. For instance, the presence of “double-ended comedones”—two blackheads that appear connected under the skin—is a hallmark sign of follicular remodeling and hyperkeratosis.
Furthermore, the symmetry of the lesions is a major clue. If you have recurring “boils” in both armpits or both sides of the groin, it is almost certainly not a random infection. It is a systemic susceptibility of the hair follicles in those regions. Identifying these patterns early allows us to utilize therapies like intralesional corticosteroids or specialized laser treatments that target the follicle directly, potentially halting the triad before the rupture phase begins. This expert-led approach is what differentiates a board-certified dermatologist from general care.
Therapeutic Interventions: Halting the Triad’s Progression
Treating HS effectively requires a multi-pronged approach that addresses each part of the follicular occlusion triad in Hidradenitis Suppurativa. We don’t just treat the symptoms; we target the mechanism. This requires a shift from short-term relief to long-term follicular stability.
Specifically, our treatment protocols focus on the following three pillars:
- Reducing Hyperkeratosis: We utilize topical retinoids and specific washes (like resorcinol) to thin the follicular lining and prevent the initial keratin plug from forming.
- Controlling the Immunological Explosion: For patients with frequent ruptures, we use systemic medications like biologics (TNF-alpha inhibitors) to dampen the immune system’s overreaction. This prevents the massive abscesses that follow a follicular breach.
- Structural Management: Once tunnels have formed, medical therapy alone is often insufficient. We may use “deroofing” procedures—a surgical technique that opens the tunnels and allows them to heal from the bottom up—to remove the “tunnels of despair” permanently.
Moreover, lifestyle factors like weight management and smoking cessation are not just general advice; they are critical because both obesity and smoking increase mechanical friction and pro-inflammatory cytokines, directly feeding into the triad’s cycle. Therefore, every action you take should be viewed through the lens of: “Does this help stabilize my hair follicles?”
The Path Forward: 5 Steps to Manage Follicular Occlusion Today
If you suspect you are dealing with the follicular occlusion triad in Hidradenitis Suppurativa, waiting for the “next boil to go away” is a dangerous strategy. Progression is the enemy. Follow these five clinical steps to regain control of your skin health.
Step 1: Document the Pattern. Stop looking at individual bumps. Note the locations and the frequency. Are they in the same spots? Do they happen in both armpits? This data is crucial for your dermatologist to confirm the triad rather than a simple infection.
Step 2: Eliminate Friction. Wear loose-fitting, breathable clothing made of natural fibers. Friction acts as a mechanical trigger for follicular rupture. Reducing the physical stress on your follicles can significantly lower the frequency of flares.
Step 3: Refine Your Skincare. Avoid harsh scrubs or heavy oils in intertriginous areas. These can worsen hyperkeratosis. Use gentle, antiseptic cleansers as directed by a specialist to manage the bacterial load without irritating the follicular wall.
Step 4: Seek Specialist Diagnosis. Consult a board-certified dermatologist who understands the nuances of HS. Standard clinics may prescribe endless rounds of antibiotics that don’t address the underlying follicular failure. Early specialized intervention is the only way to avoid surgery later.
Step 5: Address Systemic Triggers. If you smoke, seek support to quit immediately. If you have hormonal imbalances (like PCOS), address those concurrently. HS is a systemic disease with a cutaneous manifestation; treating the body as a whole is pivotal for success.
By following this methodical approach, you move from being a passive sufferer to an active manager of your condition. For personalized guidance in Antalya, you can contact Dr. Ebru Okyay to begin your clinical roadmap to remission.
Frequently Asked Questions (FAQs)
What is the very first sign of the follicular occlusion triad in Hidradenitis Suppurativa?
The earliest sign is often infundibular hyperkeratosis, which appears as small, firm blackheads (comedones) or recurring red bumps in areas like the armpits or groin. Unlike regular pimples, these bumps tend to recur in the exact same spot and may feel deeper under the skin, signaling the initial follicular blockage.
Why do my HS lesions always turn into tunnels and scars?
Tunnels, or sinus tracts, form during the third phase of the follicular occlusion triad. When the hair follicle ruptures internally, the body tries to heal by growing a skin lining around the inflammation. This creates permanent subcutaneous channels. Early treatment focuses on preventing the rupture to avoid this irreversible structural damage.
Is the follicular occlusion triad caused by poor hygiene?
No, this is a common myth that delays diagnosis. The follicular occlusion triad in Hidradenitis Suppurativa is a structural and immunological issue rooted in genetics, hormones, and follicular fragility. It has nothing to do with how often you bathe. Scrubbing the area too hard can actually trigger more ruptures and worsen the condition.
How does smoking affect the follicular occlusion triad?
Smoking is one of the most significant external triggers for HS. Nicotine and other chemicals promote hyperkeratosis (thickening of the follicle lining) and increase the release of pro-inflammatory cytokines. This makes the follicles more likely to clog and more prone to violent ruptures when they do, significantly accelerating disease progression.
Can laser hair removal help with the follicular occlusion triad?
Yes, laser hair removal can be a methodical part of treatment for many HS patients. By destroying the hair follicle entirely, we remove the structure where the triad begins. Without a follicle to clog or rupture, the cycle of inflammation is broken. However, this should only be done under the supervision of a dermatologist specializing in HS.

