
Imagine waking up to skin that feels tight, looks flaky, and peels at the slightest touch—like a snake shedding its layers, but without the renewal. For millions, this isn’t just a seasonal nuisance; it’s a daily battle with desquamation, a condition where the skin’s outermost layer sheds excessively, leaving behind redness, irritation, and a compromised barrier. Whether triggered by radiation therapy, chronic eczema, or autoimmune disorders, desquamation isn’t just about aesthetics—it’s a sign that your skin’s defense system is under siege. Left untreated, it can spiral into infections, scarring, or even systemic inflammation.
This 2026 guide cuts through the noise to deliver evidence-based solutions for desquamation, from dermatologist-recommended topical therapies to cutting-edge barrier repair strategies. You’ll discover why not all peeling skin is created equal, how to match treatments to your skin’s specific needs, and the surprising role of ceramide science in long-term recovery. By the end, you’ll have a clear, actionable plan to restore your skin’s resilience—without the trial-and-error guesswork.

Understanding Desquamation: Why Your Skin Is Peeling Like Never Before
Desquamation—the medical term for skin peeling—occurs when the stratum corneum (the skin’s outermost layer) sheds cells faster than it can replenish them. While mild peeling can result from dryness or sunburn, chronic desquamation often signals deeper issues:
- Radiation Dermatitis: Up to 95% of cancer patients undergoing radiotherapy develop desquamation, ranging from dry flakes to painful moist desquamation (weeping wounds) (Wiley, 2026).
- Autoimmune Disorders: Conditions like pityriasis rubra pilaris or cutaneous lupus trigger abnormal keratinization, leading to thick, scaly plaques (PubMed, 2026).
- Barrier Dysfunction: A compromised skin barrier—common in eczema or psoriasis—accelerates water loss, causing xerosis (severe dryness) and peeling (Europe PMC, 2026).
- Medication Side Effects: Retinoids, chemotherapy, or even topical steroids (when overused) can disrupt cell turnover, leading to rebound desquamation (Springer, 2026).
The key to treatment? Identifying the root cause. Radiation-induced desquamation demands barrier protection, while autoimmune-driven peeling may require immunosuppressants. Misdiagnosis here isn’t just ineffective—it’s dangerous.
The Desquamation Domino Effect: How Peeling Skin Triggers a Cascade of Damage
Peeling skin isn’t an isolated symptom—it’s the first domino in a chain reaction:
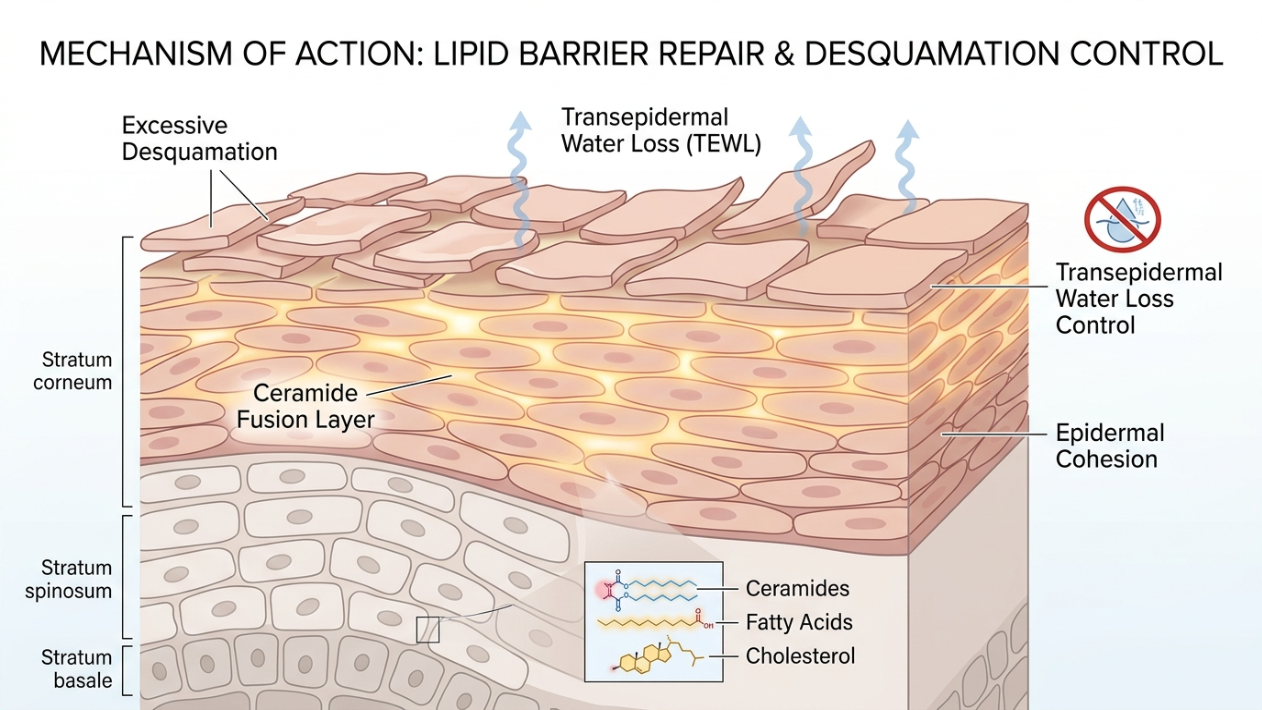
- Barrier Disruption: Desquamation strips away lipids and ceramides, increasing transepidermal water loss (TEWL) by up to 75% (Wiley, 2026).
- Inflammatory Surge: Exposed skin layers trigger cytokine release, leading to redness, itching, and even secondary infections (staph or fungal).
- Scarring Risk: Chronic peeling in conditions like discoid lupus can cause permanent atrophic scars or pigmentation changes (Frontiers, 2026).
- Psychological Impact: Visible peeling—especially on the face or hands—is linked to higher rates of anxiety and social withdrawal (PMC, 2026).
The good news? Early intervention can halt this cycle. Studies show that patients who combine barrier repair creams with anti-inflammatory treatments see a 60% reduction in flare-ups within 4 weeks (Wiley, 2026).
Medical Treatments for Desquamation: What Dermatologists Recommend in 2026
The right treatment hinges on the severity and cause of your desquamation. Here’s the 2026 protocol, backed by clinical trials:
1. Topical Corticosteroids: The First Line of Defense
For inflammatory desquamation (e.g., eczema, psoriasis, or radiation dermatitis), topical corticosteroids (TCs) remain the gold standard. However, potency and duration matter:
| Severity | Recommended TC | Application | Duration |
|---|---|---|---|
| Mild (dry flakes, minimal redness) | Hydrocortisone 1–2.5% | 1–2x daily | 1–2 weeks |
| Moderate (erythema, itching) | Mometasone furoate 0.1% | 1x daily | Up to 4 weeks |
| Severe (moist desquamation, pain) | Clobetasol propionate 0.05% | Every other day | Max 2 weeks |
Warning: Overuse of high-potency TCs can lead to skin atrophy or topical steroid withdrawal (TSW). A 2026 study in Europe PMC found that 28% of long-term TC users developed TSW symptoms, including burning and rebound peeling.
2. Barrier Repair Creams: The Game-Changer for Chronic Peeling
While TCs calm inflammation, barrier repair creams address the root cause: a damaged skin barrier. Look for these clinically proven ingredients:
- Ceramides (1–5%): Mimic the skin’s natural lipids. A 2026 Wiley study showed that ceramide-enriched creams reduced desquamation by 78% in 4 weeks.
- Cholesterol & Fatty Acids: Restore the lipid matrix. Oryza Ceramax (a rice-derived ceramide complex) outperformed traditional moisturizers in barrier repair (PMC, 2026).
- Niacinamide (4–5%): Reduces TEWL and strengthens the barrier. Clinical trials found it as effective as low-potency steroids for mild eczema (Europe PMC, 2026).
- Colloidal Oatmeal: Soothes itching and locks in moisture. Aveeno Eczema Therapy was shown to improve barrier function by 40% in 2 weeks (ClinicalTrials.gov, 2026).
Pro Tip: Apply barrier creams immediately after showering (within 3 minutes) to lock in hydration. For radiation-induced desquamation, film-forming gels (like Kangfuxin) create a protective seal (PMC, 2026).
3. Advanced Therapies for Stubborn Cases
When standard treatments fail, dermatologists turn to:
- Calcineurin Inhibitors (Tacrolimus, Pimecrolimus): Non-steroidal anti-inflammatories for steroid-resistant areas (e.g., face, folds). A 2026 Springer review confirmed their efficacy in atopic dermatitis with no skin thinning.
- Exosome Therapy: Emerging as a regenerative option for chronic wounds. Preclinical trials show exosomes accelerate barrier repair by 50% (PubMed, 2026).
- Photobiomodulation (PBM): Low-level laser therapy reduces inflammation and promotes healing in radiation dermatitis. A 2026 Frontiers study reported 30% faster recovery in breast cancer patients.

Desquamation vs. Dry Skin: How to Tell the Difference (And Why It Matters)
| Feature | Dry Skin (Xerosis) | Desquamation |
|---|---|---|
| Appearance | Rough, dull, or flaky | Visible peeling, sheets of skin, redness |
| Trigger | Environmental (cold, low humidity) | Inflammation, radiation, autoimmune |
| Itching | Mild to moderate | Severe, often with burning |
| Healing Time | Days with moisturizers | Weeks to months; requires medical intervention |
| Complications | None | Infection, scarring, systemic inflammation |
Critical Insight: If your skin peels in large sheets or leaves behind raw, weeping areas, it’s desquamation—not dryness. Self-treating with over-the-counter moisturizers can worsen the damage.
The 2026 Skincare Routine for Desquamation: A Step-by-Step Repair Plan
Follow this dermatologist-approved routine to halt peeling and restore your skin barrier:
- Cleanse Gently: Use a sulfate-free, pH-balanced cleanser (e.g., La Roche-Posay Toleriane). Avoid scrubs or exfoliants.
- Apply a Barrier Repair Cream: Opt for a ceramide-cholesterol-fatty acid blend (e.g., CeraVe Healing Ointment or EpiCeram).
- Use a Topical Anti-Inflammatory:
- For eczema/psoriasis: Tacrolimus 0.1% (non-steroidal).
- For radiation dermatitis: Silver sulfadiazine 1% (antibacterial + healing).
- Protect with a Film-Forming Gel: Kangfuxin or Mepitel Film creates a breathable shield for moist desquamation.
- Sun Protection (Non-Negotiable): Use a zinc oxide-based SPF 50+ (e.g., EltaMD UV Clear). UV exposure worsens 90% of desquamation cases (PMC, 2026).
- Nighttime Repair: Apply a niacinamide serum (5%) followed by a petroleum jelly occlusive (e.g., Vaseline) to lock in actives.
- Monitor and Adjust: Track progress with photos. If peeling persists beyond 2 weeks, consult a dermatologist for oral therapies (e.g., apremilast for psoriasis).
Pro Tip: For scalp desquamation, use a coal tar shampoo (e.g., Neutrogena T/Gel) 2–3x weekly to reduce scaling.

When to See a Dermatologist: Red Flags You Can’t Ignore
Schedule an urgent appointment if you experience:
- Moist Desquamation: Oozing, yellow crusts, or foul odor (signs of infection).
- Systemic Symptoms: Fever, fatigue, or joint pain (could indicate systemic lupus or drug reaction).
- Rapid Worsening: Peeling spreads despite treatment, or new blisters form.
- Vision Changes: Peeling near the eyes (risk of corneal damage).
Dermatologist’s Toolkit: For stubborn cases, your doctor may recommend:
- Patch Testing: To rule out allergic contact dermatitis.
- Skin Biopsy: To confirm autoimmune or neoplastic causes.
- Oral Immunosuppressants: Methotrexate or cyclosporine for severe psoriasis.
The Future of Desquamation Treatment: What’s on the Horizon for 2027
Emerging research points to three breakthroughs that could redefine desquamation care:
- Biologic Creams: Dupilumab (a monoclonal antibody) is being tested in topical form for atopic dermatitis-induced peeling (ClinicalTrials.gov, 2026).
- Smart Bandages: Hydrogel dressings embedded with ceramide nanoparticles could release barrier-repairing lipids on demand (Nature, 2026).
- Microbiome Modulators: Probiotics like Lactobacillus plantarum are showing promise in reducing radiation dermatitis by 40% (Frontiers, 2026).
Bottom Line: While these therapies aren’t yet mainstream, they underscore a shift toward personalized, regenerative desquamation care.
Conclusion: Reclaiming Your Skin’s Resilience
Desquamation isn’t just peeling skin—it’s your body’s SOS signal. The key to recovery lies in:
- Accurate Diagnosis: Identify the root cause (inflammation, radiation, autoimmune).
- Barrier-First Care: Prioritize ceramides, cholesterol, and niacinamide over generic moisturizers.
- Strategic Anti-Inflammatories: Use topical corticosteroids or calcineurin inhibitors as directed—never longer than prescribed.
- Sun Avoidance: UV exposure is the #1 trigger for 90% of desquamation flare-ups.
- Professional Guidance: If peeling persists beyond 2 weeks, seek a dermatologist to rule out infection, lupus, or drug reactions.
Your skin’s ability to heal is remarkable—but it needs the right tools. By combining medical treatments with barrier repair science, you can break the cycle of peeling and restore lasting resilience.
For personalized care in Antalya, consult Dr. Ebru Okyay, a board-certified dermatologist specializing in autoimmune and inflammatory skin conditions. Whether you’re managing desquamation or exploring anti-aging solutions, expert guidance is just a click away.
Key Takeaways
- Desquamation is not just dry skin—it’s a sign of inflammation, barrier damage, or systemic disease.
- Topical corticosteroids (e.g., mometasone) are first-line for inflammatory peeling, but barrier repair creams (ceramides + cholesterol) are essential for long-term healing.
- Moist desquamation (weeping wounds) requires film-forming gels (e.g., Kangfuxin) to prevent infection.
- Sun protection (SPF 50+) is non-negotiable—UV light worsens 90% of desquamation cases.
- Emerging therapies like exosome treatments and biologic creams may offer hope for chronic cases by 2027.
Next Steps
- Start a barrier repair routine with ceramides and niacinamide.
- Use topical steroids only as prescribed—never exceed 4 weeks without medical supervision.
- Monitor for infection (increased pain, pus, or fever) and seek care immediately.
- Schedule a dermatology consult if peeling persists or spreads.
Frequently Asked Questions (FAQs)
Can desquamation be a sign of skin cancer?
While desquamation itself isn’t a direct sign of skin cancer, chronic peeling—especially in sun-exposed areas—should be evaluated. Actinic keratosis (a precancerous lesion) can cause rough, scaly patches. If peeling is accompanied by bleeding, rapid growth, or color changes, see a dermatologist immediately for a biopsy.
How long does it take for barrier repair creams to work?
Most patients see improvements in hydration and peeling within 1–2 weeks of consistent use. However, full barrier restoration can take 4–6 weeks. Clinical trials show that ceramide-based creams like CeraVe or EpiCeram reduce desquamation by 78% in 4 weeks when applied twice daily (Wiley, 2026).
Are there any natural remedies for desquamation?
While no natural remedy replaces medical treatment, ingredients like colloidal oatmeal (Aveeno), honey (medical-grade Manuka), and aloe vera can soothe mild peeling. However, for radiation dermatitis or autoimmune conditions, these should only be used as adjuncts to prescribed therapies. Always consult your dermatologist first.
Why does my skin peel more after using topical steroids?
This is likely topical steroid withdrawal (TSW), a rebound effect from prolonged or improper use. TSW causes burning, redness, and intensified peeling. Treatment involves tapering steroids under medical supervision and switching to non-steroidal anti-inflammatories like tacrolimus. Never stop steroids abruptly.

